
In this blog series we take a deeper look into particular anatomical variations to celebrate their uniqueness as well as shine a spotlight on potential issues they may cause.
We are all unique in the way we look, think and behave, and so is our anatomy. Yes, we have organs in common, but their shape and position can vary from individual to individual.
This article on coronary artery anatomical variations will explore the anatomy and physiology of the heart, the arterial supply via the coronary arteries, the variations that can occur and the relevant clinical factors.
By the way, are you a coronary artery? ‘Cause you’re wrapped all around my heart!
Anatomy and physiology of the heart
The cardiovascular system consists of the heart, blood vessels (arteries, veins and capillaries) and blood. The heart acts as a pump, ensuring that blood circulates through every blood vessel in the body, supplying cells with the oxygen and nutrients they need to survive.
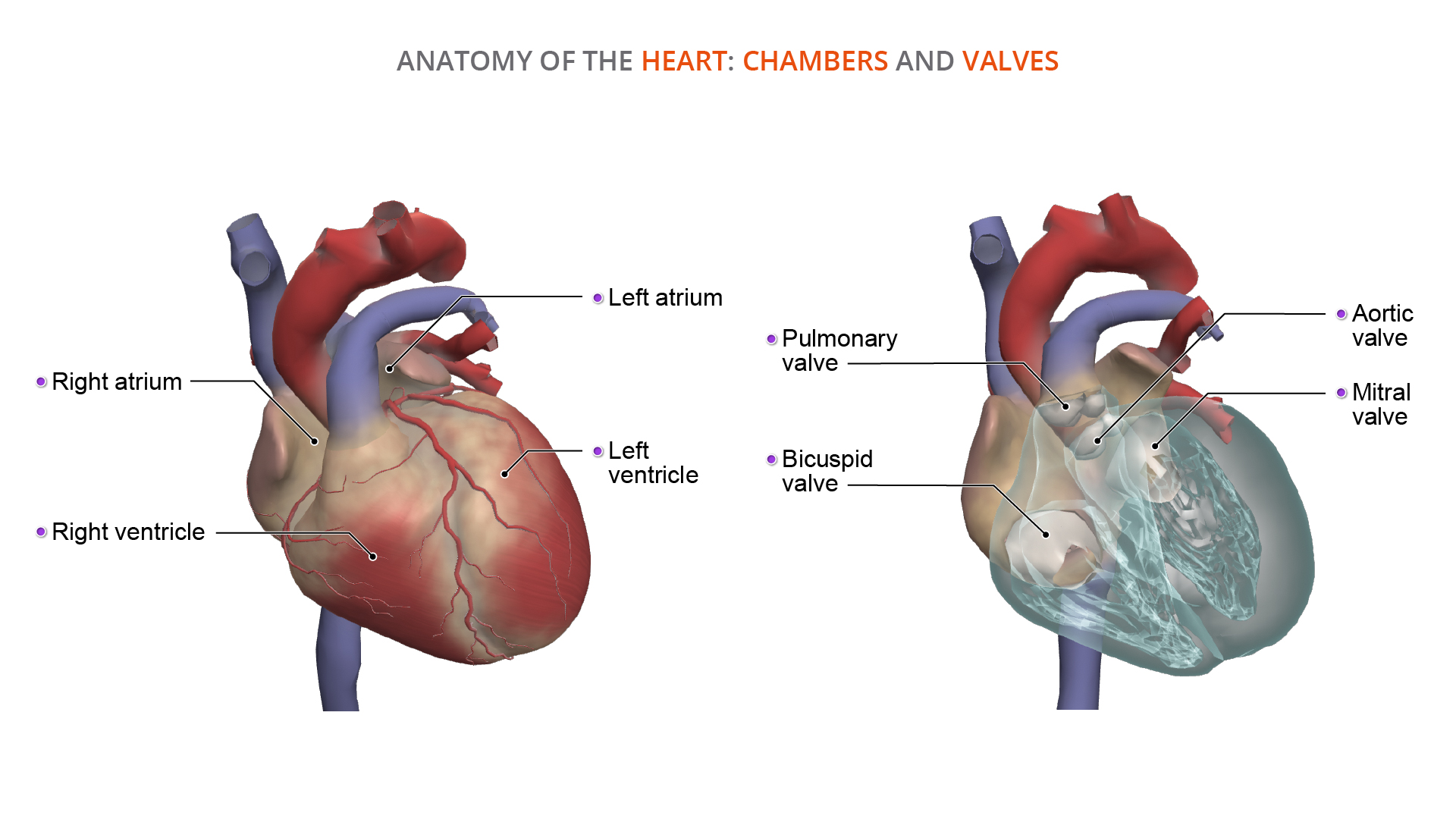
The heart is made up of:
- Four chambers: atria and ventricles
- Muscular wall: encasing the atria and ventricles
- Muscular septum: separating the atria and ventricles into right and left sides
- Four valves:
- The mitral and aortic valves let oxygenated blood flow through the left heart chambers to the rest of the body
- The bicuspid and pulmonary valves let deoxygenated blood flow through the right heart chambers to the lungs
- Conduction system: two nodes act as natural pacemakers and set the heart rhythm by innervating a network of nerves
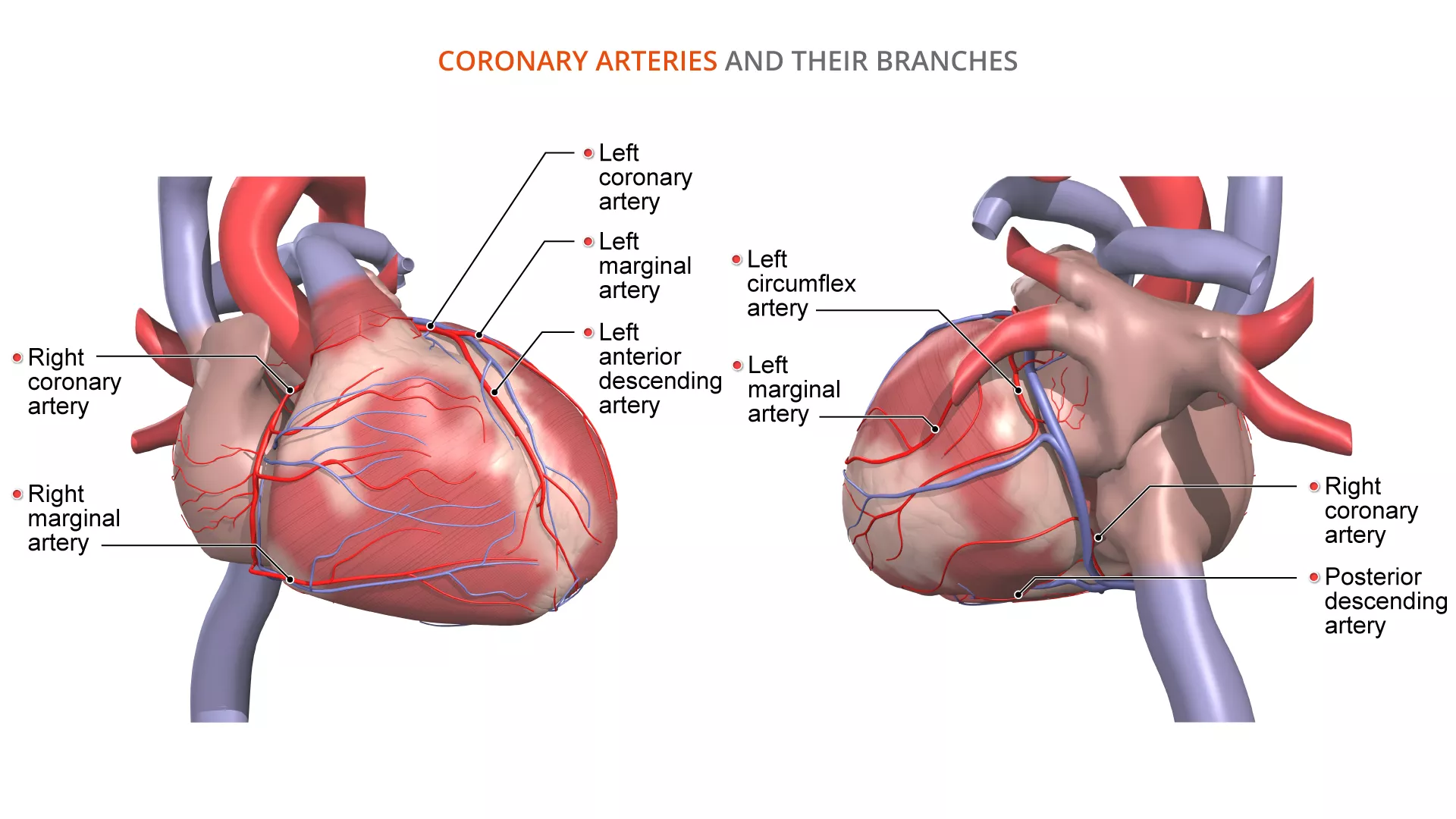
Coronary arteries
The heart has its own blood supply through the coronary arteries to receive oxygen and nutrients that will allow it to pump effectively.
The coronary arteries branch off from the aorta, just above the left ventricle, into a left and right coronary artery. They further branch around the heart and communicate with each other by joining (anastomosing) together to form continuous loops. This is very important if one of the vessels becomes blocked, as it provides an alternative route for blood to supply the muscles of the heart.
The left coronary artery has the following branches:
- Left circumflex artery
- Left anterior descending artery/anterior interventricular artery
- Left marginal artery
The right coronary artery has the following branches:
- Posterior descending artery/posterior interventricular artery
- Right marginal artery
In the above branching pattern, the left coronary artery supplies:
- The left atrium
- Both left and right ventricles
- The muscular septum
And the right coronary artery supplies:
- The right atrium
- The right ventricle
- The nodes in the conduction system
Coronary artery variations
The majority of people have the coronary arteries branching as above, with the right coronary artery giving rise to the posterior descending artery (~80%). These individuals are known as right dominant.
Sometimes the branching pattern of the left and right coronary arteries differ from above and, in these cases, are known as variations. The most common variations are:
- Left dominant (in ~10% of people)
- Balanced (codominant) (in ~10% of people)
In left dominant cases the posterior descending artery branches from the left coronary artery instead of the right via the left circumflex artery, or less commonly by the left anterior descending artery.
In balanced or codominant cases, the posterior descending artery is a formed by the left circumflex artery and the right coronary artery joining together, so both coronary arteries supply the posterior descending artery.
Why it’s important to know about variations in the arterial supply of the heart
It’s important to understand the variations of the coronary arteries in case either the right or left coronary artery becomes blocked. In right dominant cases, if the right coronary artery is blocked, this means blood can’t reach the posterior descending artery and important structures like the conducting nodes will fail to function, resulting in the heart failing to pump.
However, in a left dominant case, if the right coronary artery is blocked, there won’t be a disruption of blood supplying the conducting nodes because the posterior descending artery branches from the left coronary artery.
Surgical procedures and coronary artery variations
Understanding these variations are immensely helpful to clinicians planning interventional procedures to treat coronary artery disease, particularly when there are secondary changes of calcification, plaque formation and stenosis.
Treatments for coronary artery disease include:
- Balloon angioplasty: A balloon is inflated inside the blocked artery to increase blood flow.
- Coronary artery stent: A tiny mesh coil is expanded inside the blocked artery to keep the pathway open.
- Atherectomy: Using a device on the end of a catheter to cut away plaque from the artery wall.
- Laser angioplasty: Light is used to remove blockages in the coronary artery.
- Coronary artery bypass: Grafting a portion of vein above and below the artery to bypass the blockage. (Veins are usually from the leg, but can be from the chest or arm. Sometimes multiple bypass procedures need to be in place to allow the blood to flow fully to the heart.
The images used in this piece have been taken from Primal’s Anatomy & Physiology and 3D Real-time modules. To learn more about this or other Primal digital content – please fill in the form here and our team will be in touch.